An educational guide for patients with drug-resistant epilepsy: when surgery
is considered, how candidates are evaluated, and how the modern view of
seizures as a network problem is changing surgical planning.
Overview
When epilepsy surgery is considered
Epilepsy is a disorder in which the brain produces recurrent, unprovoked seizures.
For most people with epilepsy, anti-seizure medications control seizures well enough
to allow a normal life. For roughly one in three patients with focal epilepsy,
however, two or more well-chosen medications fail to control seizures. This
condition is called drug-resistant epilepsy (also termed
refractory or pharmacoresistant epilepsy), and it is where surgical evaluation
becomes relevant.
The goal of epilepsy surgery is to identify the region of brain tissue from which
seizures originate — the epileptogenic zone — and to
either remove it, destroy it, or modulate the network that supports it, while
preserving function. When the epileptogenic zone is well-defined and lies in
non-eloquent tissue, surgery can produce sustained seizure freedom in a substantial
proportion of patients. When the zone is diffuse or close to function-critical
cortex, the surgical options are different but still meaningful.
This site is a patient-education resource from Dr. Atik's University of Chicago practice. It does not replace evaluation by a comprehensive epilepsy center.
Evaluation
How candidates are evaluated
Comprehensive epilepsy surgery evaluation is a stepwise process. Each step
narrows the question: is there a single, surgically accessible region driving
the seizures, and can it be treated without unacceptable functional cost.
01
Phase I — Non-invasive
Long-term video-EEG monitoring with scalp electrodes, high-resolution MRI, neuropsychological testing, and often PET, ictal SPECT, and MEG. The goal is concordant evidence pointing to a single brain region.
02
Patient management conference
A multidisciplinary team — epileptologists, neurosurgeons, neuropsychologists, neuroradiologists — reviews all data and decides whether the candidate proceeds directly to surgery, requires invasive monitoring, or is not a surgical candidate.
03
Phase II — Invasive monitoring
When non-invasive data is insufficient, intracranial electrodes record directly from the brain. Two main approaches: SEEG (depth electrodes placed through small drill holes, ideal for deep or bilateral sampling) and ECoG (subdural grids on the cortical surface, ideal for mapping eloquent areas).
04
Surgical planning
Once the epileptogenic zone is localized, the team plans the specific procedure: resection, ablation, disconnection, or neuromodulation. Modern planning increasingly incorporates network-level analysis and structural connectivity mapping.
Seizure networks
Seizures as a network, not a single spot
For decades, epilepsy surgery was framed around the seizure-onset zone: find
the single piece of cortex where seizures start, remove it, and the patient
becomes seizure-free. This works in some patients. In many others —
especially those with normal MRIs or prior failed surgery — the picture
is more complicated.
Contemporary research describes focal epilepsy as a network
disorder. Seizures originate at an onset region but recruit a broader set of
connected nodes through white matter pathways. Some of those nodes participate
actively in the seizure even though they appear quiet under conventional
thresholds. Mapping this network — both the onset zone and the
propagation regions, and the structural tracts that connect them — is
an active area of clinical research.
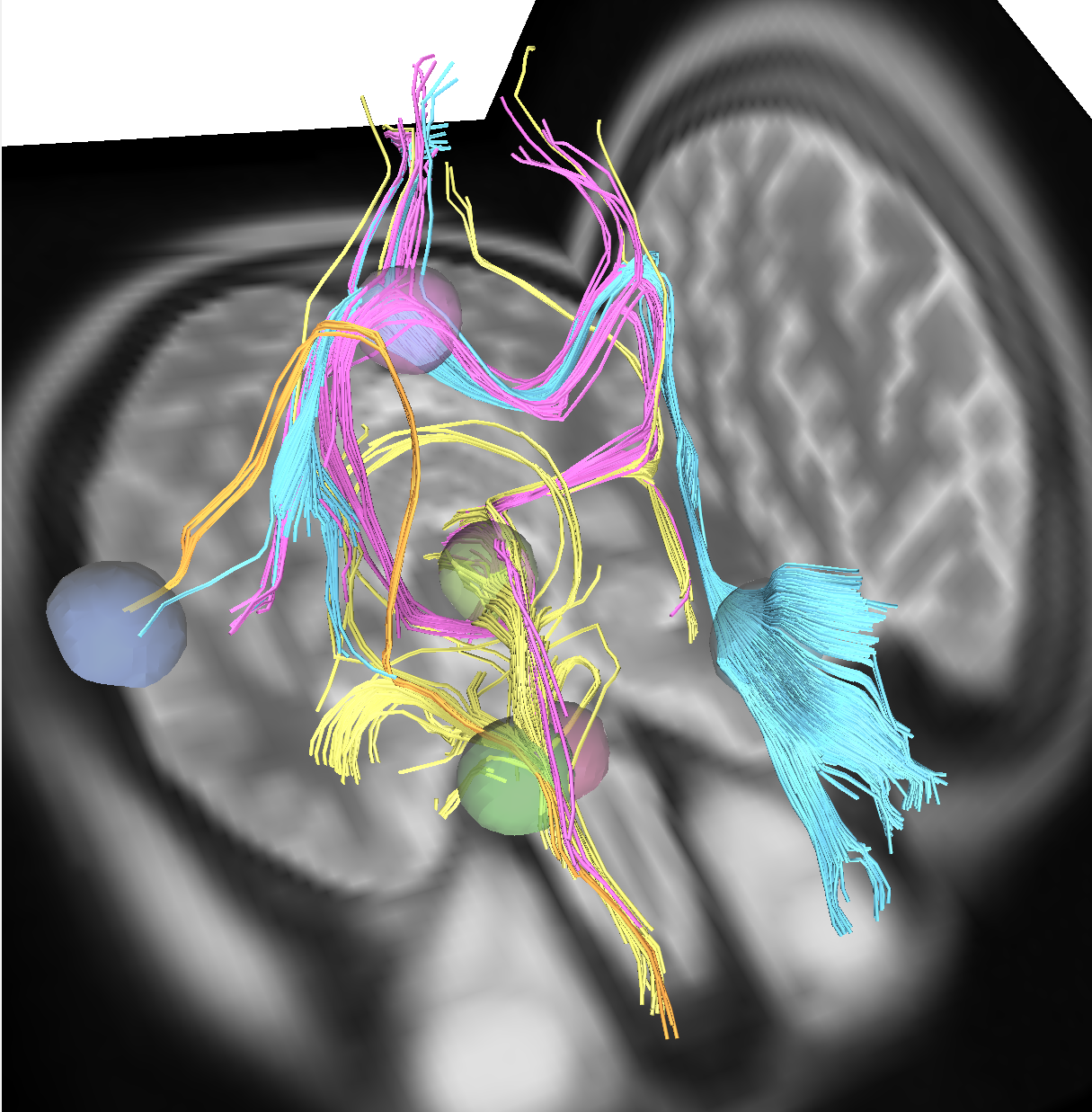
Network mapping
Seizure network with structural connectivity
A reconstruction of the seizure-onset zone and propagation regions identified from intracranial EEG, with the white matter tracts connecting them.
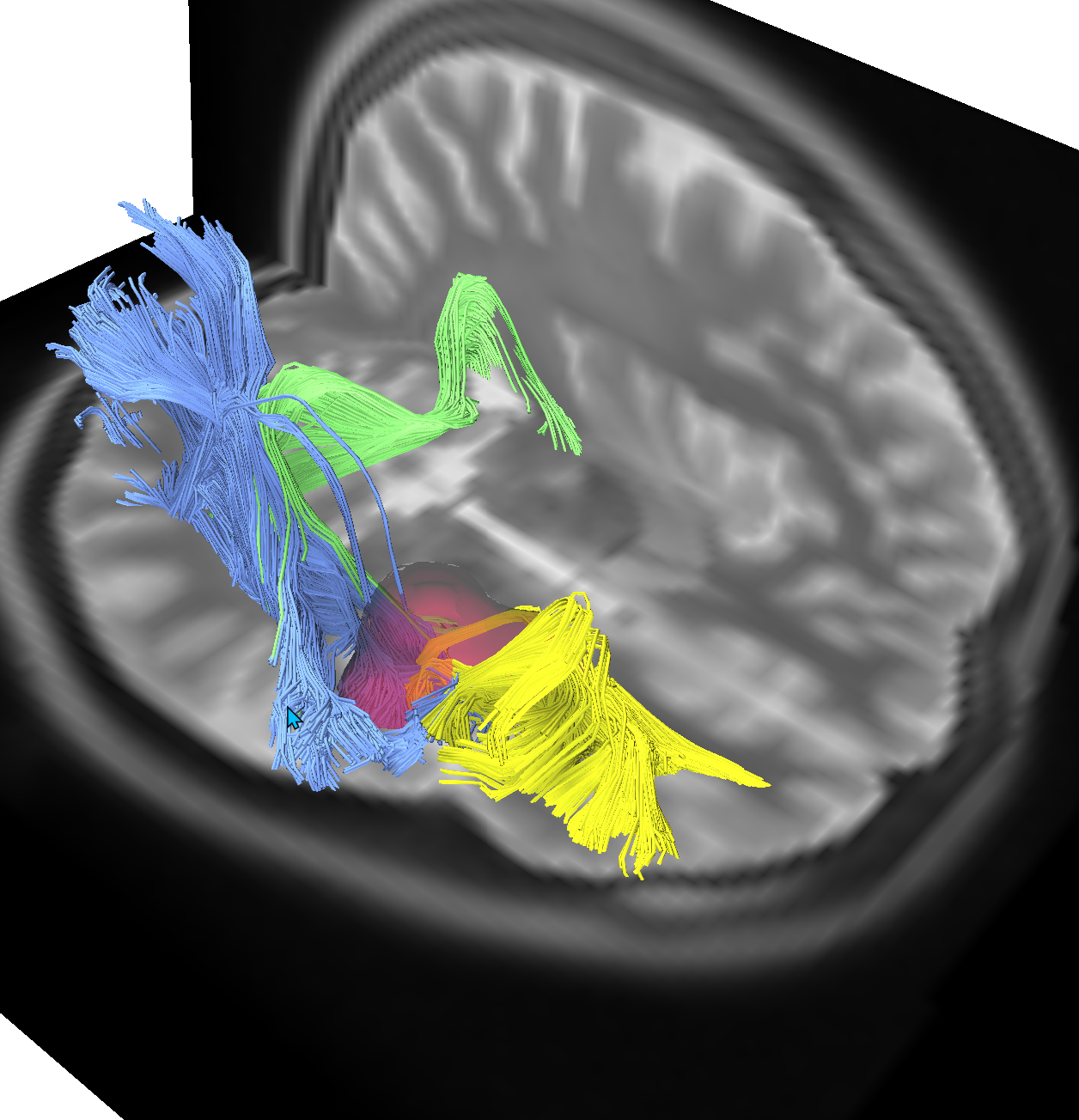
Tractography
Eloquent pathway mapping around a lesion
White matter tracts reconstructed around a lesion to identify the safe surgical corridor and the pathways that must be preserved during resection.
Procedures
Types of epilepsy surgery
There is no single "epilepsy surgery." The surgical options span removing
epileptogenic tissue, disconnecting it from the rest of the brain, destroying
it with heat or radiation, and modulating the network with implanted devices.
The procedure is chosen based on the location of the epileptogenic zone, its
relationship to eloquent cortex, and the patient's specific clinical picture.
Each option below is described for orientation; choice belongs to the patient's
own epilepsy team.
Resective Surgery
Selective Amygdalohippocampectomy (SAH)
Targeted removal of the amygdala and hippocampus through a limited approach, sparing the lateral temporal neocortex. Performed via transsylvian, subtemporal, or transcortical corridors depending on the dominant white matter anatomy and vascular relationships.
Anterior Temporal Lobectomy (ATL)
Resection of the anterior temporal lobe including the mesial structures. The standard surgical treatment for mesial temporal lobe epilepsy when the temporal pole and lateral cortex are part of the epileptogenic network.
Tailored Cortical Resection
Individually designed resection of focal epileptogenic cortex, guided by SEEG or subdural grid mapping. The resection boundaries are shaped by the seizure onset zone, early propagation, and proximity to functional cortex.
Lesionectomy with Functional Margin Mapping
Removal of a discrete structural lesion (tumor, cavernoma, FCD) with tractography-informed margins. White matter mapping defines the safe boundary between lesion and eloquent pathways.
Extratemporal Lobe Resection
Resection of epileptogenic cortex in the frontal, parietal, or occipital lobes. Requires precise delineation of the seizure network relative to motor, sensory, language, and visual pathways.
Insular Resection
Surgical access to the insula through a transsylvian approach for insular-onset epilepsy. Technically demanding due to proximity to the MCA branches, lenticulostriate arteries, and the internal capsule.
Hemispheric & Disconnection
Open Hemispherectomy (Delalande Technique)
A vertical parasagittal hemispherotomy performed through a limited craniotomy. Disconnection of the affected hemisphere through the lateral ventricle, sectioning the corona radiata, corpus callosum, and fornix while preserving vascular structures.
Vertical Hemispherotomy (Lateral Approach)
Hemispheric disconnection via a lateral transcortical route through the superior temporal gyrus or peri-insular corridor. Access to the ventricle allows callosotomy, fornix section, and disconnection of the frontal and occipital horns.
Peri-Insular Hemispherotomy (Superior Approach)
Access through the superior circular sulcus of the insula. A supragaleal approach to the ventricle providing disconnection of the hemisphere through the internal capsule and callosal fibers with minimal cortical removal.
Functional Hemispherotomy
Complete disconnection of one hemisphere while leaving the cortical mantle in situ. Achieves the seizure control of anatomic hemispherectomy with lower complication rates by avoiding the large resection cavity.
Corpus Callosotomy
Partial (anterior two-thirds) or complete section of the corpus callosum to prevent bilateral seizure generalization. Primarily used for drop attacks and atonic seizures in patients who are not candidates for focal resection.
Multiple Subpial Transections (MST)
Vertical cuts through the cortex at 5mm intervals to disrupt horizontal fiber connections while preserving columnar organization and function. Used in eloquent cortex where resection would cause unacceptable deficit.
Stereotactic placement of a laser fiber into the target under real-time MRI thermometry. Controlled thermal ablation of mesial temporal structures, hypothalamic hamartomas, or deep focal lesions through a single burr hole.
Radiofrequency Thermocoagulation via SEEG Electrodes
Bipolar RF energy delivered between adjacent SEEG contacts during the monitoring phase. Creates small lesions at the seizure onset zone without additional surgery. Can serve as both a diagnostic and therapeutic intervention.
Stereotactic Radiofrequency Ablation
Percutaneous or frame-based RF probe placement to create targeted thermal lesions. Used for periventricular nodular heterotopia and other deep targets not amenable to open resection.
Responsive Neurostimulation (RNS)
A closed-loop implanted device that detects seizure-onset electrographic patterns and delivers targeted electrical stimulation to abort the seizure. Placed directly at the seizure focus with cortical strip or depth leads.
Deep Brain Stimulation (DBS, Anterior Nucleus of Thalamus)
Bilateral stereotactic implantation of DBS electrodes in the anterior thalamic nucleus. Open-loop scheduled stimulation modulates the thalamocortical network to reduce seizure frequency in drug-resistant focal epilepsy.
Vagus Nerve Stimulation (VNS)
Implantation of a pulse generator connected to the left vagus nerve in the neck. Delivers intermittent stimulation to modulate brainstem and cortical excitability. A palliative option for patients not candidates for resective or ablative surgery.
Which procedure is right for a given patient
Selecting among these procedures is a clinical decision made by a
multidisciplinary epilepsy team based on the patient's seizure semiology,
imaging findings, intracranial monitoring results, neuropsychological
profile, and goals of care. Different procedures suit different network
anatomies and different relationships to eloquent cortex; no single
approach is superior in isolation.
Research
What the data so far suggests
Network-level analysis of intracranial-EEG recordings is an active area of
clinical research. One line of work, conducted by the author of this site on
publicly available stereo-EEG and ECoG datasets, characterizes a class of
propagation regions that conventional energy thresholds tend to miss:
56
Patients analyzed
5
Medical centers
91%
Showed propagation regions
p<10−6
Cross-method agreement
These observations are research findings on retrospective public datasets,
not a claim of clinical benefit. They are described in more technical detail
at neuroniuminstitute.com.
Tools in development
The Neuronium System
Research-stage seizure-network analysis
The Neuronium System is a research-stage analysis pipeline developed by the
author of this site at the Neuronium Neuroscience Institute. It combines
three layers of analysis: (1) identification of the seizure-onset zone from
intracranial EEG, (2) detection of additional propagation regions that
conventional energy thresholds may attenuate, and (3) projection of both
onto the patient's white matter via tractography for surgical review.
It is not a treatment, not a medical device approved by the FDA, and not yet
in routine clinical use. It is mentioned here for transparency, because the
research figures shown above derive from this work. Technical detail and the
underlying methods paper are available at
neuroniuminstitute.com.
Step 1 — Onset detection
Z-scored energy methods localize the seizure-onset zone from raw intracranial recordings — the conventional starting point.
Step 2 — Propagation regions
A dual-metric ranking surfaces "energy-dominant" regions whose absolute ictal energy exceeds their normalized expression and which standard thresholding may attenuate.
Step 3 — Tractography integration
Tractography reconstructs the white matter tracts connecting onset and propagation regions, projected into a single three-dimensional view for review.
About the author
Who wrote this site
AFA
Ahmet Fatih Atik, MD
Neurosurgeon · stereotactic and functional neurosurgery
Dr. Atik is a neurosurgeon whose clinical practice focuses on
stereotactic and functional neurosurgery, including the surgical
treatment of drug-resistant focal epilepsy — resection,
laser ablation, intracranial monitoring (SEEG, ECoG), and
neuromodulation (RNS, DBS, VNS).
Alongside clinical work, he conducts independent research on
network-level analysis of intracranial EEG and on the integration
of structural connectivity into surgical planning. This research
program is housed at the Neuronium Neuroscience Institute, an
independent research entity.
This site is the patient-education resource of Dr. Atik's practice at the University of Chicago Department of Neurosurgery. It does not constitute medical advice, and viewing it does not by itself establish care; a clinician-patient relationship begins at a scheduled visit.
Further reading
Authoritative resources for patients
The following organizations publish patient-facing material on epilepsy and
epilepsy surgery that is freely available and independent of this site.
Professional society publishing the international classification of seizures and consensus guidelines that frame current clinical practice.
Contact
Questions or feedback
If something on this site is unclear, incorrect, or could be explained better
for patients and families, please write. Inquiries from journalists, clinicians,
and researchers are also welcome.